
Stening® Class LSD Stent
Code CLASS LSD

Description
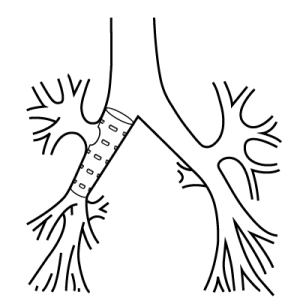
The Stening® Class LSD Stent is a device designed to maintain the clearance of the airway in sufficient conditions for ventilation. It has a side hole that allows ventilation of the right upper lobe.
It has a conical elastic tubular structure, with non-slip spurs arranged in several rows and distributed symmetrically along its surface.
Special features:
To accompany the functionality of the bronchus and its physiology, the strength of its wall is progressively reduced distally at a rate of 3% per each centimeter of the length of the stent.
Although the increase in the fixing capacity of the Stening® Class LSD Stent can not be precisely determined with regard to its counterpart, this property is benefited by the existence of fixations aligned against the direction of possible unwanted displacement. Their number duplicates the existing ones in the straight stent model.


| References | Dimensions (mm) | |||||
|---|---|---|---|---|---|---|
| Translucent | Radiopaque | Length (L) | Larger diameter (A) | Wider wall (B) | Narrower wall (C) | Smaller diameter (D) |
| CLASS-LSD10-30 | CLASS-LSDX10-30 | 30 | 10 | 1.1 | 0.9 | 9.1 |
| CLASS-LSD10-40 | CLASS-LSDX10-40 | 40 | 10 | 1.1 | 0.9 | 8.8 |
| CLASS-LSD10-50 | CLASS-LSDX10-50 | 50 | 10 | 1.1 | 0.9 | 8.5 |
| CLASS-LSD11-30 | CLASS-LSDX11-30 | 30 | 11 | 1.1 | 0.9 | 9.9 |
| CLASS-LSD11-40 | CLASS-LSDX11-40 | 40 | 11 | 1.1 | 0.9 | 9.4 |
| CLASS-LSD11-50 | CLASS-LSDX11-50 | 50 | 11 | 1.1 | 0.9 | 9 |
| CLASS-LSD12-30 | CLASS-LSDX12-30 | 30 | 12 | 1.2 | 1 | 10.9 |
| CLASS-LSD12-40 | CLASS-LSDX12-40 | 40 | 12 | 1.2 | 1 | 10.4 |
| CLASS-LSD12-50 | CLASS-LSDX12-50 | 50 | 12 | 1.2 | 1 | 10 |
| CLASS-LSD13-30 | CLASS-LSDX13-30 | 30 | 13 | 1.3 | 1.1 | 11.8 |
| CLASS-LSD13-40 | CLASS-LSDX13-40 | 40 | 13 | 1.3 | 1.1 | 11.4 |
| CLASS-LSD13-50 | CLASS-LSDX13-50 | 50 | 13 | 1.3 | 1.1 | 11 |
| CLASS-LSD14-30 | CLASS-LSDX14-30 | 30 | 14 | 1.4 | 1.2 | 12.8 |
| CLASS-LSD14-40 | CLASS-LSDX14-40 | 40 | 14 | 1.4 | 1.2 | 12.4 |
| CLASS-LSD14-50 | CLASS-LSDX14-50 | 50 | 14 | 1.4 | 1.2 | 12 |
For custom made devices you can contact us
Due to the characteristics of the production process,
the sizes of the devices may vary by +/- 2%
- Bronchial neoplasms
- Neoplasms in right or intermediate source bronchus that do not affect the upper lobe
- Neoplasms that invade tracheal carina or its slopes
- Impending atelectasis
- Following laser photorecorder, cryotherapy or electrocautery, to maintain the opening of the airway
- Bronchial stenosis
- Postinfectious stenosis (tuberculosis, histoplasmosis with mediastinal fibrosis, herpes virus, diphtheria)
- Post-traumatic stenosis
- Post-terminal surgical bronchial anastomosis stenosis
- Bronchial rupture
- Extrinsic compression
- Bronchomalacia
- Bronchial Amyloidosis
- Excessive dynamic compression of the airway
- Invasion of bronchial sources by esophageal carcinoma
- After endoscopic resection of bronchial metastases
- Medical grade silicone
- Bevelled edges to prevent granulomas
- Spur system to prevent migration
- Removable
- Surface of maximum softness to avoid adherence of secretions
- Transparent or Radiopaque
Introduction technique:
The procedure will be carried out under general anesthesia.
The implantation of this type of prosthesis requires the use of a conventional introducer for silicone prostheses. The airway will be accessed with a rigid bronchoscope. The length and clearance of the trachea or bronchus in the segment in which the stent will be housed must be estimated in order to make the correct choice of prosthesis.
Retrograde Implant Mode:
- Lubricate the nozzle of the introducer, preventing the lubricant from reaching the operator’s fingers.
- Fold the Stening® Class LSD over its axial axis and insert it into the prosthesis introducer through the mouthpiece, with the narrowest end of the stent in the distal position.
- Remove the nozzle.
- Pass the injured area with the bronchoscope tube and locate its distal end or bevel on the healthy mucosa, exceeding the affected area by 5 to 7 mm.
- Place the introducer inside the bronchoscope.
- Press the ejector while extracting the bronchoscope in equal measure in which the plunger progresses inside. The prosthesis will be released. If necessary, it can be accommodated with a crocodile clip, the manoeuvre being simpler if the stent is “lower” than the lesion.
Antegrade mode of implant:
Steps 1,2 and 3 will be repeated.
Now stop the bronchoscope containing the introducer and the prosthesis, 5 mm before the lesion to be treated. Then slowly press the ejector plunger. In this way the prosthesis will advance inside the bronchial area to be treated.
A prosthesis magazine can be used to then propel it through the interior of the bronchoscope or the method that the operator deems preferable.
Correcting the position of the stent:
The stent may require additional manoeuvres in order to correct or adjust its final position. It is preferable to correct a stent that has been installed beyond the desired position, which is the other way round, as it is highly inconvenient to advance a prosthesis that has been released before the lesion to be treated.
To mobilize a stent proximally, it can be taken from the edge and gently pulled. We strongly recommend by precise, a manoeuvre that consists of taking the stent by its edge as mentioned. Then introduce the direct vision optics inside the stent and observe its final end. Now pull the clamp and you can verify the stent’s rise inside the bronchus. Stop traction then when you think the stent location is optimal.
LSD models may require a “rotation” adjustment, so that the lateral hole of the stent faces the entrance to the right upper lobe bronchus.
Extraction technique:
The intubation will be carried out with a rigid bronchoscope.
A simple way of extraction, the stent must be taken by its edge with a crocodile forceps, with enough steadiness. Rotate the forceps so that the stent is omega-shaped and loses its radial resistance to compression. Next, pull the clamp by removing the prosthesis together with the bronchoscope. If you prefer, you can insert the end of the stent into the endoscope. With this manoeuvre the vocal cords are protected during the extraction.
- Maintain the moisture of the secretions when they exist, performing frequent nebulizations with warm isotonic saline solution
- Periodic control according to medical criteria.
- Treat dental caries and perform effective oral hygiene
The Stening® Class LSD Stent is an anatomical, slightly conical stent, therefore:
- Remember that the stent should always be inserted into the bronchoscope with the larger diameter end in a proximal position, and the narrowest end in distal one.
- If it is necessary to shorten the stent, it is preferable to make the cut close to its distal end. In other words, near the end of the smaller diameter.
- As the name implies, LSD models are only useful in the right hemi-tree. In Class LSD models, when loading the stent into the introducer or the bronchoscope, remember to orient the lateral hole of the stent towards the entrance of the right upper lobe bronchus, which is usually at 3 o’clock. Check this location previously during the Bronchoscopic examination and once again after the implant.
- The device should not be reused.
A sterile non-bioabsorbable tubular device intended to be implanted into the trachea and/or a bronchus/bronchiole to maintain luminal patency, typically used in cases of obstructions/stenoses, fistulae, tumours, scarring, surgical resection and anastomosis, or pulmonary transplantation. It is made entirely of a synthetic polymer(s) [e.g., silicone] and may have various designs (e.g., semi-soft continuous tube, covered or non-covered mesh structure, straight or branched configuration) intended to conform to the endotracheal/endobronchial surface. It may be expandable in situ (e.g., self-expands) and disposable devices intended to assist implantation may be included.
46977
